In a previous blog post, we compared documenting in spreadsheets, the EHR, and OncoNav. While spreadsheet documentation can be a quick way to document and track patient data, it is often difficult to standardize, share, and compile in a way that effectively shows the benefit of the navigation program. In this next part of our blog post series, we’re going to further compare documenting in the EHR and OncoNav so that you can decide which documentation platform would work best for you.
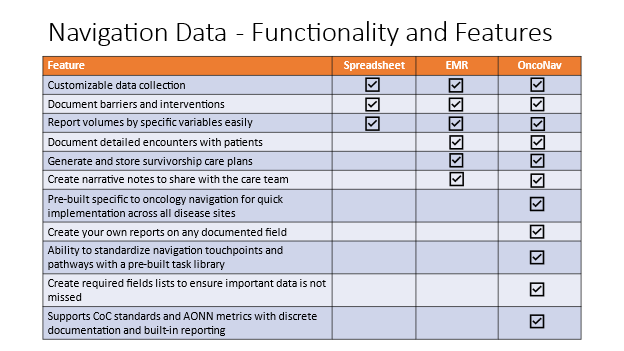
Comparison graphic
Document detailed encounters with patients
When navigators meet with patients, they want to document that visit or call so they have a timeline of that patient’s navigator care. In the EHR, the navigator may have a customized location to document those encounters in a flowsheet. They may also write a brief narrative note of that encounter. Most often, this information is completely up to the navigator for what is included and how it is written leading to a lack of standardization.
OncoNav uses a calendar feature where navigators can add those encounters for that patient. Those encounters for the navigator’s patients will also display in the navigator’s own calendar. The encounters, or tasks, have names that quickly provide more information about that visit. The navigator may be meeting with the patient to provide treatment education or information about survivorship. Additionally, the navigator can add any new or edit any existing barriers to care and interventions in that encounter. Finally, the navigator can write that brief note in the encounter itself. Any note in the patient’s OncoNav record can be exported to the EHR using the included Notes interface to ensure that all the members of the patient’s cancer healthcare team can see these encounters with navigation.
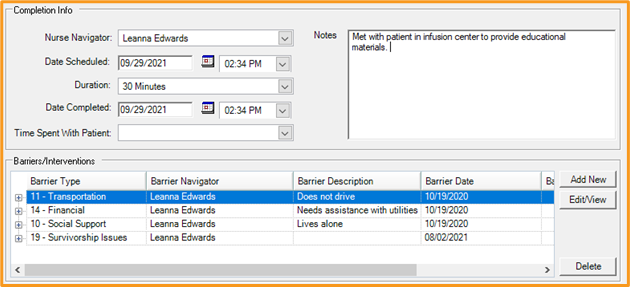
Document patient encounters in OncoNav
Generate and store survivorship care plans
OncoNav supports several of the Commission on Cancer (CoC) standards including Standard 4.8: Survivorship Program. As part of this standard, many cancer programs continue to provide survivorship care plans. Some cancer programs have been able to build out documentation and reporting to support survivorship care plans in their EHR. Those that have been successful in doing so were likely not without their fair share of hardships added as part of any customization in the EHR, including time constraints and available resources. Creating the survivorship care plan in the EHR does not necessarily allow easy reporting of the number of patients who received them.
OncoNav includes pre-built templates that support both ASCO and NCCN recommendations to allow for easy creation of the survivorship care plan with the simple click of a button. Completed treatment information can be brought into the care plan from the facility’s cancer registry, and other information is populated from data items documented in OncoNav. The survivorship care plan can then be saved to the patient’s OncoNav record and transmitted back to the EHR to share with the rest of the health care team. OncoNav allows the navigator to quickly document that the survivorship care plan was provided, as well as any other service provided to the patient in survivorship for easier tracking and reporting.
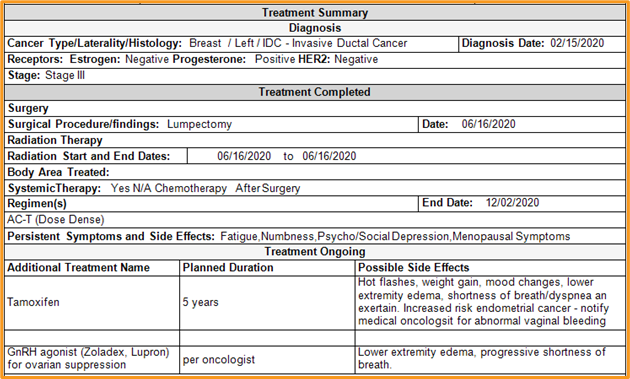
SCP snippet in OncoNav
Create narrative notes to share with the care team
Navigators meet with patients to discuss and educate on the diagnosis, the treatment plan, and survivorship, all while assessing barriers to care. Navigators often write a narrative note in their EHR of what occurred during that visit or phone call so that other members of the patient’s healthcare team know what the navigator is doing with the patient. Documentation can differ navigator to navigator and these notes are no different. While navigators may have the ability to pull in some documented data into the EHR narrative note, there is often no standardization to that narrative. Those who may be well versed in the EHR may be able to create a template which will then have to be manually shared to others in their navigation team.
OncoNav includes pre-built narrative note templates that offer the ability for the navigator to create the note with pre-populated data such as treatment information, any barriers discovered, and the interventions provided. This note can then be transmitted back into the EHR for the rest of the healthcare team to understand the navigator’s role in the patient’s cancer care. With these narrative notes stored in one place in OncoNav, the navigator and care team can very quickly glance at the history of navigation with this patient. These note templates help to standardize documentation for the navigation program rather than having one navigator write a quick one line note and another writing a full-page document.
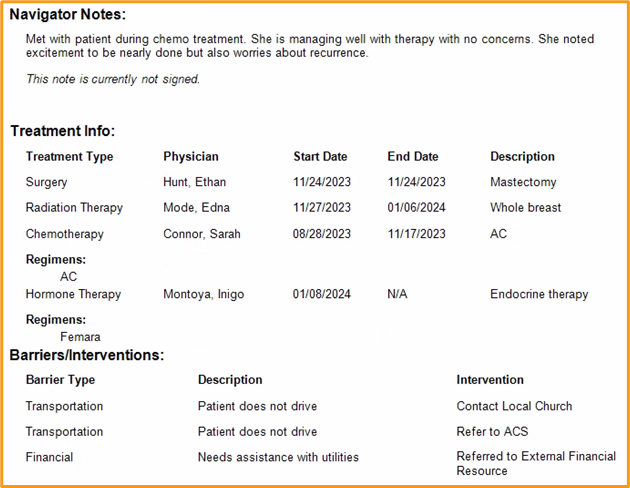
Partial navigator note in OncoNav
Our final post in this series will continue in the next few weeks to explore why OncoNav is the premier platform for oncology navigation documentation and reporting. For more information about oncology navigation documentation with OncoNav, please reach out to us at support@onco-nav.com. If you’re not a current client and would like to see a demo, please email us at sales@oncolog.com or click the link Schedule a Demo from the Onco website.

Oncology Data Management Software That Makes a Difference.
Enhance workflows while delivering quality information.